INTRODUCTION
Sports performance, as a multifactorial process, is directly and indirectly influenced by a wide range of components of sports preparation, classified in the theory and methodology of sports training into major areas of intervention, such as physical, psychological, socioeconomic, medico-biological, and pedagogical, among others. Therefore, the analysis of sports performance is based on a comprehensive approach, as defined by Gómez-Ruano et al.(1). Specifically, muscle recovery and sleep hygiene have emerged as fundamental components for optimizing sports performance in terms of supercompensation, as an indicator directly related to organic bioadaptation(2,3), and the prevention of sports injuries(4,5).
In specific disciplines such as volleyball, characterized by explosive and repeated high-intensity efforts with brief recovery periods(6), sleep represents a significant physiological resource that still requires scientifically grounded integration and monitoring within educational and specialized training programs, particularly in youth categories(7,8).
Sleep hygiene refers to a set of behavioral and environmental practices aimed at promoting optimal nocturnal rest. These include maintaining regular sleep schedules, avoiding excessive screen use before bedtime, ensuring an appropriate sleep environment, and reducing or eliminating the consumption of stimulants such as caffeine(9). In a sports context, poor sleep hygiene has significant repercussions on sleep quality, which in turn negatively affects physiological recovery, hormonal balance, cognitive function, and the consolidation of effective motor learning habits(10,11). These alterations can directly impact the athlete’s physical, psychological, and technical performance(12,13), including youth volleyball players(14,15), an age group that also faces additional challenges related to biological maturation, academic stress, and competitive pressures.
On the other hand, muscle recovery, as a biological process, involves the reconstruction of muscle fibers, including the reabsorption of metabolites and the restoration of energy balance(16). This process is enhanced by sleep as a recovery mechanism, which is planned according to the principle of the appropriate balance between load and rest(17,18). During deep sleep phases, particularly slow-wave sleep, there is an increase in growth hormone secretion, protein synthesis, and modulation of biological inflammation(19,20). Therefore, lack of sleep delays these restorative processes and increases the risk of overload injuries, a relatively common issue in systematically trained volleyball players.
Although existing research strongly supports the essential role of sleep-in organic recovery and, consequently, in sports performanc (21,22), there remains a practical need to pedagogically implement sleep hygiene strategies in training programs for youth athletes. This is particularly relevant given that families, coaches, and athletes themselves often tend to underestimate the importance of nocturnal rest compared to other performance-related variables such as nutrition, socio-familial stability, training load variation, or game tactics(23). This tendency is especially concerning during adolescence, a critical stage for neurobiological and psychological development(24).
Based on the above, there is a need to design specialized educational intervention strategies for the organization and structuring of volleyball training components(25,26), including aspects such as sleep hygiene and general muscle recovery. These strategies should be adapted to the psychosocial characteristics of youth volleyball players, promoting autonomous and sustainable practices that positively impact overall health and, consequently, the athlete’s career trajectory. In this regard, various studies report educational interventions on sleep with positive outcomes in sleep quality and duration, as well as in related variables such as physical performance and attention(27,28).
In some invasion sports such as basketball and football, similar program focused on muscle recovery and sleep hygiene have been shown to improve reaction times, mood, and perceived exertion(29,30), all of which are also relevant indicators in volleyball. However, the national and international literature reviewed does not provide sufficient evidence of specific program targeting youth volleyball players, thereby justifying the theoretical and methodological relevance of the present study.
This research will not only contribute to filling a gap in the scientific literature applied to volleyball but will also serve as a theoretical and methodological basis for designing future educational policies and preventive strategies in school, federated, and community sports contexts. Therefore, the aim of this study is to analyze the effects of an educational program for youth volleyball players on sleep hygiene and muscle recovery.
METHODS
The study used a quasi-experimental design with a pretest–posttest approach and an equivalent control group, based on the hypothesis that “an educational program adapted to the needs of youth volleyball players will improve sleep hygiene and muscle recovery.” The dependent variables were “sleep hygiene” and “muscle recovery,” while the independent variable was “the educational program.”
A representative sample of male youth volleyball players (U18/U19) was studied, selected through unrestricted random sampling (N=57; confidence: 95%; error: 5%; n=50), and divided into two independent groups of equal size (n=25 each). This sample size was sufficient to establish reliable correlations with a medium effect size (Cohen’s d: 0.50), a significance level of 0.05, and statistical power of 1 – β error probability (0.80). The inclusion criteria describing the study population were:
- Youth volleyball players according to International Volleyball Federation standards (U18/U19), male, and members of provincial teams in the Republic of Cuba.
- Regular competitive activity with scientifically trained teams (at least five previous years).
- Minimum training load (≥ 4 weekly sessions or ≥ 8 hours/week).
- Compatible health status and absence of recent sports injuries.
- No use of self-medicated or prescribed pharmacological treatments affecting sleep or recovery.
- Availability and ability to comply with at least 90% of the intervention process, and signed informed consent.
The Sleep Hygiene and Muscle Recovery Educational Program (PHS-RM) was implemented over eight consecutive weeks, aiming to improve nocturnal sleep habits and optimize muscle recovery in youth volleyball players. The intervention included:
- Theoretical-practical educational sessions.
- Standardized sleep hygiene routines.
- Post-training muscle recovery components.
- Weekly monitoring and feedback.
The intervention group followed the proposed program, while the control group continued with their usual sports training plan. The implementation phases were:
- Familiarization Phase (Week 0): Initial orientation session (90 min): Explanation of the study objective, benefits of sleep for performance and muscle recovery, instructions for daily sleep tracking and the TQR scale. Distribution of printed and digital materials: illustrated guides with sleep hygiene routines (schedules, bedroom environment, screen and caffeine restrictions), stretching techniques, and a daily log. Baseline assessment as part of the pretest, which included sleep quality, perceived muscle recovery, and supplementary data such as morning heart rate, total sleep time, and perceived muscle fatigue.
- Educational Phase (weeks 1-2): two in-person group sessions (60 min each, once a week) led by a sleep medicine specialist and a physical trainer, which included: Session 1: fundamentals of sleep and performance (chronobiology, sleep stages, relationship with protein synthesis and recovery, and importance of consistent schedules/going to bed between 10:00-11:00 pm, waking up between 6:30-7:00 am). Session 2: sleep hygiene applied to athletes (control of light and ambient temperature (18-20 °C), limiting screen time ≥ 60 min before bed, reducing caffeine and energy drinks after 4:00 pm, breathing relaxation techniques and gentle stretching before bed; the sessions included practical demonstrations of relaxation and stretching routines.
- Structured intervention phase (weeks 3-8): Includes a daily sleep hygiene routine (fixed bedtime (10:30 PM ± 30 min) and wake-up time (6:45 AM ± 30 min), avoiding naps longer than 30 min and after 5:00 PM, use of dim light (≤ 50 lux) one hour before sleep, nighttime practice of 5-7 min of diaphragmatic breathing and gentle dynamic stretching of the lower and upper body. Post-training muscle recovery routine applied immediately after each volleyball session in ≥ 3 sessions/week (guided hydration (7-10 ml/kg within 30 min after training), sequence of static stretches held for 15-20 s per muscle group (shoulders, back, quadriceps, hamstrings, calves, lumbar erectors), use of self-massage with a foam roller for 5 min (2 slow passes per group)). muscle. Recording of the level of perceived recovery using TQR 30 min after the session).
- Monitoring and feedback phase: (includes a sleep diary) nightly recording of bedtime, wake-up time, nighttime awakenings, and naps. Weekly follow-up by the principal investigator was also conducted to address questions, verify adherence, and reinforce habits, along with personalized feedback for each player based on the diary entries and the TQR (Treatment Questionnaire). Adherence was defined as ≥ 80% compliance with daily routines and in-person sessions. Adherence was verified through review of sleep diaries and session attendance, and players with < 80% adherence were analyzed according to the intention-to-treat principle but reported as under-adherent.
- Final evaluation phase (post-test/week 8): re-application of PSQI, TQR, sleep diaries and other secondary variables. Intra-group (pre- vs post-) and inter-group (experimental vs control) comparison to determine the effects of PHS-RM.
Players in the experimental group showed high adherence to the PHS-RM program (≥90%), indicating its feasibility and acceptance in a youth sports context. Participants with lower adherence were included in the analysis under the intention-to-treat principle.
The volleyball players in the experimental group showed a high degree of adherence to the PHS-RM, according to the adherence analysis. Adherence was operationally defined as the execution of at least 90% of the daily intervention routines, attendance at face-to-face educational sessions, and continuous implementation of post-training muscle recovery strategies. This was confirmed through weekly analysis of sleep diaries, TQR records, and participation in scheduled sessions. Most members of the experimental group reached appropriate adherence standards (≥90%), indicating that the program is accepted and feasible in a youth sports setting. To maintain the internal validity of the study, participants with lower levels of adherence were included in the analysis according to the intention-to-treat principle, without being excluded from the statistical processing.
The study complied with international ethical guidelines for human research (CIOMS, 2016) and received institutional ethics committee approval. Informed consent was obtained from parents/guardians, and assent from the players. The following internationally validated instruments were used:
- Pittsburgh Sleep Quality Index (PSQI): a 19-item questionnaire that assesses sleep quality over the past month, plus five additional items to be answered by a bed partner. (31) Dimensions: subjective sleep quality; sleep latency (time to fall asleep); sleep duration; usual sleep efficiency (hours slept/hours in bed); sleep disturbances (awakens, breathing problems, nightmares, etc.); use of sleep medication; daytime dysfunction (sleepiness, fatigue). Norms: each dimension is scored from 0 to 3 (0 = no problem; 3 = severe problem; 0-4: good sleep quality; 5-10: poor sleep quality; >10: significant sleep disturbances). The overall score is obtained by summing the seven components, with a range of 0 to 21 points.
- Total Quality Recovery Scale (TQR): assesses muscle recovery and fatigue through a “perceived recovery” dimension, validating the level of recovery and perceived fatigue after training sessions or competition. (32) The scale consists of a single item: “How would you rate your overall recovery (physical and mental) since the last training session/competition?” Norms: the athlete indicates a value on a Likert-type scale of 6 to 20 points (6–10: very poor to poor recovery (high fatigue); 11–14: moderate recovery; 15–17: good recovery; 18–20: very good/optimal recovery.)
Data did not follow a normal distribution according to the Shapiro-Wilk test (p < 0.05). Therefore, non-parametric statistics were used: Wilcoxon signed-rank test for related samples and Mann–Whitney U test for independent samples (p ≤ 0.05). Statistical analyses were conducted using IBM SPSS Statistics and G*Power.
RESULTS
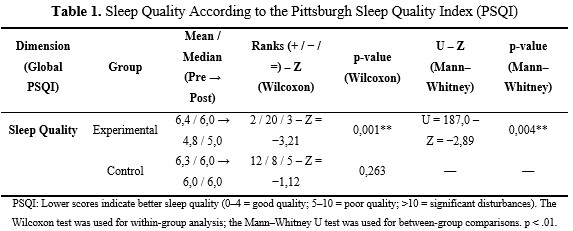
The results of the PSQI test, according to the Wilcoxon test, showed significant differences in global sleep quality for the intervention (experimental) group (p = 0.001). The mean/median scores decreased to values more consistent with a “good sleep quality” level in the posttest (mean/median: 6.4/6.0 → 4.8/5.0). Negative ranks predominated with 20 subjects (2 positive, 3 ties), and a Z value of −3.21 was reported (large effect size: r = 0.64). These results indicate a positive and consistent effect of the intervention program on sleep regulation in the volleyball players of the experimental group. In contrast, the control group showed only a slight, non-significant reduction in its global score based on central tendency data (6.3/6.0 → 6.0/6.0) and significance values (Z = −1.12; p = 0.263), maintaining a “poor” level of sleep quality. This suggests stability in the athletes’ habits in the absence of a specific intervention.
Regarding the intergroup analysis, the Mann–Whitney U test initially confirmed homogeneity between the independent groups. However, in the posttest, after the intervention, a significant difference was observed in favor of the experimental group (U = 187.0; Z = −2.89; p = 0.004), with a moderate-to-large effect size (r = 0.58). This demonstrates the effectiveness of the educational intervention program on sleep hygiene compared to the usual practice followed by the control group. (Table 1).
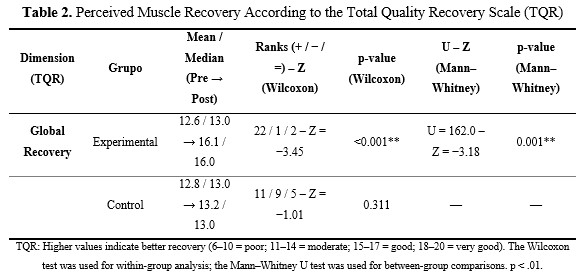
The intergroup results of the TQR test, according to the Wilcoxon test, showed that the experimental group demonstrated a significant and clinically relevant improvement at the end of the intervention. Measures of central tendency indicated a “moderate” level of recovery in the pretest (12.6/13.0), and a “good recovery” in the posttest (16.1/16.0). Rank patterns showed a predominance of positive ranks (22 positive, 1 negative, 2 ties), with a Z value of −3.45, a large effect size (r = 0.69), and high statistical significance (p < 0.001).
In contrast, the control group showed a non-significant increase in its evaluation, with lower central tendency values than the experimental group (12.8/13.0 → 13.2/13.0; Z = −1.01; p = 0.311). This suggests that the observed improvement may be attributable to normal training variations rather than a systematic effect.
Regarding the intergroup analysis, the Mann–Whitney U test showed no significant differences in the pretest, confirming initial homogeneity between the independent groups for the TQR variable. However, significant differences were found in the posttest in favor of the experimental group (U = 162.0; Z = −3.18; p = 0.001). This statistically supports the positive effects of the educational intervention program on sleep quality and the reduction of fatigue in youth volleyball players who underwent the intervention. (Table 2).
DISCUSSION
The aim of this study was to analyze the effects of a structured educational program on sleep hygiene and muscle recovery in youth volleyball players. This objective was achieved, supporting the research hypothesis that a pedagogical intervention adapted to the needs of youth volleyball players would produce significant improvements in the dependent variables compared to a control group that maintained its usual training. Significant and clinically relevant improvements were confirmed in the experimental group, both in global sleep quality and perceived muscle recovery.
From an intragroup perspective, results measured with the PSQI test showed that volleyball players who underwent the sleep hygiene and muscle recovery intervention program (PHS-RM) experienced a notable reduction in global scores, transitioning qualitatively from a “poor” level (pretest) to values consistent with a “good” level of sleep quality. This decrease was not only statistically significant but also practically relevant, as PSQI benchmarks provide clear cut-off points for clinical interpretation. In contrast, the control group maintained relatively stable values between pretest and posttest, with no significant differences, suggesting that the improvements observed in the experimental group cannot be attributed solely to natural adaptation to training or the passage of time.
These findings are consistent with the scientific literature, which highlights the positive impact of educational interventions on sleep quality in young athletes, especially those combining theoretical knowledge with practical behavioral strategies. Such interventions have been shown to improve sleep duration, regularity, and perceived quality(27,28). Similarly, Charles Walsh et al.(7) emphasize that sleep hygiene education is a fundamental tool in the comprehensive management of sports training, particularly during formative stages when habits are still modifiable.
Considering the characteristics of youth volleyball players, the observed improvements in sleep quality are particularly relevant due to the physiological and neuromuscular demands of both the sport and the athletes’ biological age. Volleyball is characterized by repeated explosive actions, such as jumps involving high-intensity efforts with short recovery periods, which require effective recovery processes(6,22). In this context, optimizing sleep facilitates key processes of supercompensation and organic adaptability, promoting better restoration of the neuromuscular system and contributing to the prevention of overload-related injuries.
The intergroup analysis further reinforced these findings. The absence of significant differences in the pretest confirmed initial homogeneity between groups, while posttest results in favour of the experimental group demonstrated the positive effect of the intervention. This pattern aligns with other studies showing that improvements in sleep quality among young athletes do not occur spontaneously but require systematic and sustained interventions(8,13).
Regarding perceived muscle recovery, TQR results showed a significant improvement in the experimental group, which progressed from “moderate” to “good recovery” levels after the intervention. This finding is particularly relevant since the TQR is widely used as a sensitive indicator of fatigue and recovery in training and competition contexts(32). The predominance of positive ranks in the Wilcoxon test, along with the magnitude of change observed, suggests that the intervention not only improved subjective perception but may also have influenced underlying physiological processes related to sleep and post-training recovery routines.
Thus, the results of this study are consistent with evidence linking adequate sleep to the optimisation of protein synthesis, hormonal regulation, and modulation of inflammatory processes, particularly during deep sleep phases(19,20). In this sense, the study provides empirical support for the inclusion of sleep hygiene educational strategies within recovery models for youth volleyball players.
Furthermore, when comparing these findings with studies conducted in other team sports, a clear convergence emerges. For example, Cheri Mah et al.(30) demonstrated that sleep extension in collegiate basketball players improved physical performance and perceived recovery, while Longo Ugolotti et al. (29) showed that sleep quality predicts perceived exertion and psychological well-being throughout a competitive season in soccer players. Although these studies were conducted in different sports contexts, their conclusions reinforce the idea that sleep is a transversal factor influencing both performance and recovery across disciplines.
Despite these findings, the study has several limitations that should be considered. The sample size, although statistically sufficient for medium effect sizes, is limited for generalizing results to other populations, such as female volleyball players or athletes from different age groups and competitive levels. Additionally, the use of subjective measures, although internationally validated, may be influenced by perceptual or motivational biases. Future studies could incorporate more objective methods such as actigraphy or polysomnography to complement these findings.
Moreover, the intervention duration of eight weeks did not allow for assessment of the long-term sustainability of the observed effects. Longitudinal studies with extended follow-up are needed to determine whether acquired habits remain effective over time and whether improvements in sleep quality and muscle recovery translate into reduced injury rates or enhanced competitive performance.
Based on these limitations, future research should expand the intervention program to different age groups and sports contexts, and analyze the specific contribution of each component (education, sleep routines, post-training recovery). It would also be valuable to explore relationships between improved sleep and key training variables such as mood, attention, technical-tactical performance, and physiological indicators of load and recovery.
In conclusion, the results of this study confirm that a structured educational intervention program targeting sleep hygiene and muscle recovery can be an effective strategy to improve rest quality and perceived recovery in youth volleyball players. These findings highlight the need to incorporate sleep as a central component in sports training management, contributing not only to athletic performance but also to health and the overall development of young athletes.
ACKNOWLEDGEMENTS
To the Teaching Innovation Project entitled: “Active methodologies for the teaching-learning process in physical education and sports” ASESDECO-PI14/22. as well as to the AFIDESA Research Group (Physical Activity, Sport and Health), of the University of the Armed Forces-ESPE.
Conflict of interest
The authors declare that they have no conflicts of interest.
Authors’ contributions
Conceptualization: Santiago Calero Morales.
Research: Santiago Calero Morales.
Data curation: Raquel Angela Olmedo Falconi, Alexandra Valeria Villagómez Cabezas, Lermay Morán Pedroso.
Formal analysis: Santiago Calero Morales, Lermay Morán Pedroso.
Methodology: Raquel Angela Olmedo Falconi, Alexandra Valeria Villagómez Cabezas.
Validation: Lermay Morán Pedroso.
Project Management: Lermay Morán Pedroso.
Acquisition of funds: Raquel Angela Olmedo Falconi, Alexandra Valeria Villagómez Cabezas.
Drafting the original: Santiago Calero Morales.
Writing, reviewing and editing: Santiago Calero Morales.
Financing
Without external financing.
REFERENCES
1.Gomez-Ruano MA, Ibáñez SJ, Leicht AS. Performance analysis in sport. Frontiers in psychology. 2020;11:611634
2.Orunbayev A. Recovery strategy in sports. American Journal Of Social Sciences And Humanity Research. 2023;3(12):135-147.
3.Amórtegui G, Álvarez A, Bermúdez E, del Pilar Gómez M, Marín M, Soto J, et al. Higiene de sueño y su impacto en los deportistas de alto rendimiento, 2022. J Health Med S. 2023;9(2):57-63.
4.Chennaoui M, Vanneau T, Trignol A, Arnal P, Gomez-Merino D, Baudot C, et al. How does sleep help recovery from exercise-induced muscle injuries? J Sci Med Sport. 2021;24(10):982-7.
5.Puga TB, Mazumder RM, Ruan T, Scigliano N, Thiel GE, Treffer K. Sleep, nutrition, hydration and rest: The equal importance of external factors outside of training and practice for sports injury prevention. Scientific Journal of Sport and Performance. 2023;2(4):428-38.
6.Venegas MP. La pliometría en el entrenamiento de la saltabilidad de los voleibolistas rematadores. Revista Conecta Libertad[Internet. 2023[citado 25/11/2025];7(2):67-85. Disponible en: https://revistaitsl.itslibertad.edu.ec/index.php/ITSL/article/view/333
7.Walsh NP, Halson SL, Sargent C, Roach G, Nédélec M, Gupta L, et al. Sleep and the athlete: narrative review and 2021 expert consensus recommendations. British J Sports Medicine. 2021;55(7):356-68.
8.Gaskin CJ, Venegas Hargous C, Stephens LD, Nyam G, Brown V, Lander N, et al. Sleep behavioral outcomes of school-based interventions for promoting sleep health in children and adolescents aged 5 to 18 years: a systematic review. Sleep Advances. 2024;5(1):zpae019.
9.Lewis LE. Sleep Your Way to Success (How to Sleep Better v2): Unlocking Your Potential Through Better Sleep and Rest. 2nd ed. Londres: Leon E. Lewis; 2024.
10.Lim ST, Kim DY, Kwon HT, Lee E. Sleep quality and athletic performance according to chronotype. BMC Sports Science, Medicine and Rehabilitation. 2021;13(1):2-15.
11.Charest J, Grandner MA. Sleep and athletic performance: impacts on physical performance, mental performance, injury risk and recovery, and mental health: an update. Sleep Medicin Cli. 2022;17(2):263-82.
12.Kaczmarek F, Bartkowiak-Wieczorek J, Matecka M, Jenczylik K, Brzezińska K, Gajniak P, et al. Sleep and Athletic Performance: A Multidimensional Review of Physiological and Molecular Mechanisms. J Clinical Medic. 2025;14(21):7606.
13.Coel RA, Pujalte GG, Applewhite AI, Zaslow T, Cooper G, Ton AN, et al. Sleep and the young athlete. Sports Health. 2023;15(4):537-46.
14.Haraldsdottir K, Sanfilippo J, McKay L, Watson AM. Decreased sleep and subjective well-being as independent predictors of injury in female collegiate volleyball players. Orthopaedic J Sports Medicine. 2021;9(9):2325-85.
15.da Silva GM, de Moura Simim MA, Nakamura FY, Coswig V, Assumpção CO, Medeiros AI. The Impact of Sleep Quality on Mood in Beach Volleyball Athletes: A Cross-Sectional Study. Retos. 2023;48:883.
16.Bazán NE. Bases fisiológicas del ejercicio (Bicolor) Barcelona: Paidotribo; 2023.
17.Gabbett TJ, Oetter E. From tissue to system: what constitutes an appropriate response to loading? Sports Medicine. 2025;55(1):17-35.
18.Balk YA, Englert C. Recovery self-regulation in sport: Theory, research, and practice. International J Sports Science & Coaching. 2020;15(2):273-81.
19.Besedovsky L, Cordi M, Wißlicen L, Martínez-Albert E, Born J, Rasch B. Hypnotic enhancement of slow-wave sleep increases sleep-associated hormone secretion and reduces sympathetic predominance in healthy humans. Communications Biology. 2022;5(1):747.
20.Lamon S, Morabito A, Arentson‐Lantz E, Knowles O, Vincent GE, Condo D, et al. The effect of acute sleep deprivation on skeletal muscle protein synthesis and the hormonal environment. Physiological Reports. 2021;9(1):e14660.
21.Orunbayev A. Recovery strategy in sports. Am J Social Sci Human Research. 2023;3(12):135-47.
22.Closs B, Burkett C, Trojan JD, Brown SM, Mulcahey MK. Recovery after volleyball: a narrative review. Physician Sports Medicine. 2020;48(1):8-16.
23.Białeta J, Rowińska K, Siembab K, Jurkiewicz M, Napieralska A, Garbarczyk W, et al. The Importance of Sleep in Athletic Performance-A Systematic Review. Quality in Sport. 2025;38:58162-5.
24.Blakemore SJ, Choudhury S. Development of the adolescent brain: implications for executive function and social cognition. Journal Child Psychology Psychiatry. 2006;47(3-4):96-312.
25.Morán-Pedroso L, Chamorro-Balseca NC, Sánchez-Córdova B, Calero-Morales S. Análisis pedagógico de las adaptaciones cardiovasculares del equipo campeón universitario de voleibol masculino. Rev Méd[Internet]. 2024[citado 25/11/2025];46:e5855.
26.Calero-Morales S, Suárez-Taboada C, Villavicencio-Álvarez VE, Mon-López D. Análisis del ranking técnico-táctico del voleibol cubano femenino, nivel escolar 2023. Arrancada[Internet]. 2023[citado 25/11/2025];23(45):151-71. Disponible en: https://revistarrancada.cujae.edu.cu/index.php/arrancada/article/view/617/411
27.Cunha LA, Costa JA, Marques EA, Brito J, Lastella M, Figueiredo P. The impact of sleep interventions on athletic performance: a systematic review. Sports Medicine-Open. 2023;9(1):58-68.
28.Merayo A, Sans O, Iranzo A, Capdevila L. Efficacy of a personalized sleep education program and its impact on academic performance in young team sports players. Apunts Sports Medicine. 2025;60(227):100483.
29.Long JW, González M, Farrell III J, Carmargo ME, Cheever K. Sleep duration and sleep quality as season-long predictors of ratings of perceived exertion and psychological well-being in female soccer athletes. J Strength & Conditioning Research. 2025;39(9):973-81.
30.Mah CD, Mah KE, Kezirian EJ, Dement WC. The effects of sleep extension on the athletic performance of collegiate basketball players. Sleep. 2011;34(7):943-50.
31.Buysse DJ, Reynolds I, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Research. 1989;28(2):193-213.
32.Coutts AJ, Slattery KM, Wallace LK. Practical tests for monitoring performance, fatigue and recovery in triathletes. J Science Medic Sport. 2007;10(6):372-81.
